
Background
Calcific tendinitis (also referred to as tendinopathy) in the shoulder is a soft-tissue pain condition involving calcium deposits in the rotator cuff tendons. The condition can present as acute or chronic. It is easily mistaken for other shoulder pathologies due to having symptoms similar to several other conditions (such as shoulder impingement, rotator cuff strain, bursitis, adhesive capsulitis (frozen shoulder), and bicipital tendinosis (possible, although not as common as the others). Let’s explore this common and painful condition more fully to know when and why, or not, to use soft-tissue therapies.
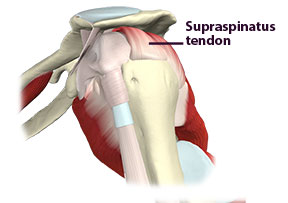
Calcific tendinitis primarily occurs in the supraspinatus tendon but can also appear in the other rotator cuff tendons. The primary issue involves calcium deposits that develop within the affected tendon. The reasons for these deposits are not firmly established yet and may involve a combination of issues.
A few various causes for this condition currently are:
- It is more prevalent in people aged 30 to 60, indicating age-related changes.
- Diabetes and thyroid disorders can increase the risk of calcium deposits in tendons, indicating metabolic disorders.
- The condition can run in families, indicating genetic predisposition.
- Repetitive stresses on the tendons (work or sports) can cause tissue damage and subsequent calcium deposits.
- Impaired blood and oxygen flow to tendons from impingement that damages capillaries or other vessels (or other injuries) can lead to tissue degeneration and calcium buildup.
- Postmenopausal women are more susceptible, suggesting hormonal influences.
- Tendon degeneration can sometimes trigger calcium deposits.
Cacific tendinitis commonly develops acutely, and people can wake up with it overnight. The condition can also come on slowly. There is no consistent pattern of occurrence. If there were, we could link more directly with a mechanical cause. Thus, it can be challenging to pinpoint the exact cause.
There may be a relationship between calcific tendinitis and other shoulder pathologies, such as subacromial impingement, but no established cause-effect connection exists. In subacromial impingement, the supraspinatus tendon is compressed against the underside of the acromion process. While compression of the supraspinatus occurs, it’s unclear whether this compression contributes to the development of the calcium deposits. It is feasible to consider that some degree of subacromial impingement might limit blood supply to the tendon and contribute to the calcification.
There does seem to be an active inflammatory process with calcific tendinitis, although it is not fully understood. Some cases exhibit active inflammation, which may either cause or result from calcium deposit formation. Because anti-inflammatory medications provide pain relief, it suggests an inflammatory component.
These calcifications can spontaneously reabsorb without any intervention in some cases. When the cases resolve on their own, the tendon tissue gradually returns to normal as the deposits dissolve. However, the healing process is disrupted in chronic calcific tendinitis, leading to prolonged symptoms and potential continued calcium deposit formation.
Assessment
Differentiating calcific tendinitis from other shoulder pathologies is essential for proper treatment or referral. Because there is bone calcification in the tendon, x-ray evaluation is commonly used to identify the problem. Ultrasound and MRI are also used. While imaging techniques are helpful, proper identification still relies heavily on the client history and physical examination. Therefore, it is valuable for massage therapists to understand some of the key clinical characteristics of this condition. Here are some of the key characteristics that clients can present with:
- Rapid onset of pain: Symptoms may come on gradually or with relatively sudden onset. There is often no clear identifying trauma or injury to the area preceding the onset of pain.
2. Pain quality: Patients often describe a deep, throbbing pain similar to a toothache.
3. Pain persistence: Unlike classic impingement and tendinitis, pain may continue even with extended rest or when the shoulder is in a neutral position.
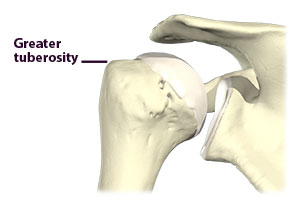
4. Pain location: Significant tenderness over the greater tuberosity of the humerus is characteristic of calcific tendinitis.
5. Pain with movement: While motion can exacerbate discomfort, pain may be present even when the arm is at rest.
6. Resisted abduction: Pain is often increased with resisted shoulder abduction.
Assessing calcific tendinitis is more of a process of exclusion. The above combination of factors should make us suspect it as a possibility. If calcific tendinitis is suspected, referring to another healthcare professional is best. Additional muscle injury could result from pressure on the calcium deposits during massage treatment.
Treatment
Treatment approaches for calcific tendinitis generally focus on conservative and non-operative methods. Here are some of the more common approaches currently used to treat the condition:
- Traditional methods: Anti-inflammatories, steroid injections, transcutaneous electrical nerve stimulation, and physical therapy show moderate benefit.
- Ultrasound therapy: Higher intensity applications have demonstrated positive results in breaking up calcium deposits.
- Extracorporeal shock wave therapy: This emerging treatment has shown promise in breaking up and dissolving calcium deposits.
- Massage therapy: The role of massage in treating calcific tendinitis remains unclear. However, without appropriate research to provide guidelines, massage is not recommended due to potential discomfort and aggravation of the condition.
- Preventive measures: Gentle range of motion exercises in non-calcified tissues may help prevent the development of secondary frozen shoulder, a potential complication of calcific tendinitis.
- Needling technique: For complicated cases unresponsive to conservative treatments, physicians may employ a needling technique to break up calcified deposits.
Calcific tendinitis is a condition that can mimic other shoulder complaints. Yet, it is a problem that should be approached cautiously from a massage perspective. Because of the potential aggravation of the complaint, it is particularly important to clarify the possible presence of the condition when considering treatment for a client that fits the symptom profile.
Want to learn more? You can learn much more about this condition and numerous other shoulder pathologies in our orthopedic massage shoulder course. Join us over there!
DE Carli A, Pulcinelli F, Rose GD, Pitino D, Ferretti A. Calcific tendinitis of the shoulder. Joints. 2014 Aug 1;2(3):130-6. doi: 10.11138/jts/2014.2.3.130. PMID: 25606556; PMCID: PMC4295680.