
The sacroiliac (SI) joint is one of the most biomechanically complex joints in the body. It is close to the body’s center of gravity and is acted on by lever forces from three directions (spine and each lower extremity). Pain may occur in the SI joint from joint pathology, such as misalignment of the rough and irregular contact surfaces between the sacrum and ilium. Pain may also occur from stresses to the many ligaments, muscles, tendons, and fascial connections in the region. Referred pain from SI joint dysfunction also accounts for a large percentage of low back pain.
This article explores important soft-tissue connections around the SI joint that involve fascia, muscles, tendons, and ligaments that all contribute to stability and proper movement.
Hamstrings to sacrotuberous ligament
The hamstrings attach through a conjoined tendon to the ischial tuberosity. However, the tendons don’t just stop at this attachment site on the ischium. There is continuity in the connective tissue of these tendons with the sacrotuberous ligament, which is oriented in the same direction as the attaching tendons (Figure 1). Anatomical studies have indicated that the fascial connections are mostly linked with the long head of the biceps femoris muscle.1
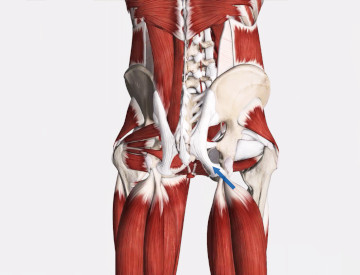
Figure 1
Hamstring tendons connect with sacrotuberous ligament
Image is from 3D4Medical’s Complete Anatomy application
The fascial connection between the hamstrings and the sacrotuberous ligament has important implications for SI joint function. There is a slight degree of motion that occurs at the SI joint called nutation and counternutation. Nutation occurs when the upper part of the sacrum tips anteriorly. Counternutation occurs when the upper border of the sacrum tips posteriorly. It may be easiest to think of this motion as a slight forward and backward rocking. The sacrotuberous ligament is attached to the lower margin of the sacrum so it becomes taut during nutation and somewhat slackened during counternutation.
Tension generated through the hamstring muscles helps to stabilize the lower margin of the pelvis. Tensile forces from the hamstrings are transmitted to the sacrotuberous ligament so it can limit nutation of the sacrum. Therefore these two structures work in conjunction with each other for proper SI joint mechanics. Conversely, if the hamstrings are hypertonic they may transmit too much tensile force to the sacrotuberous ligament causing it to pull on the sacrum and that could aggravate SI joint dysfunction.
In addition to fascial connections with the hamstrings, the sacrotuberous ligament also has fascial connectivity with the gluteus maximus muscle. The gluteus maximus plays an important role in maintaining proper stability of the SI joint because of its other fascial connections described below. Keep in mind that stresses on these fascial connections don’t have to be large forces to have an impact. Due to the rich innervation of this area, even minor tensile stress loads may cause irritation of the pain receptors and produce significant back or SI joint pain.
Thoracolumbar fascia to contralateral gluteus maximus
There is a vertical shear force on the SI joint because the contact surface between the ilium and sacrum is almost vertical and the joint supports the full upper body weight. There is a great deal of friction between the two joint surfaces to improve stability and resist the strong shear force. Unlike many other joints, the joint surfaces are rough and uneven, which helps them lock into position more effectively. The uneven surface allows them to fit together like two puzzle pieces. Stability in this region is also increased with a lateral force that squeezes the two joint surfaces together. One of the most important components to this lateral force is the coupling action of the thoracolumbar fascia from the latissimus dorsi and the gluteus maximus on the opposite side (Figure 2).
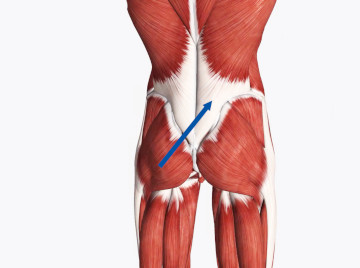
Figure 2
Thoracolumbar fascia connects with gluteus maximus
Image is from 3D4Medical’s Complete Anatomy application
Sacroiliac joint stability is greatly enhanced by having the latissimus and contralateral gluteus maximus, which are on opposite sides of the body, work together to compress the SI joint. These two muscles also work together during trunk rotation movements, which also stress the SI joints. The importance of coordinated effort between these two muscles in maintaining stability in the SI joint underscores the benefit of strength training approaches for individuals with a hypermobile SI joint. Increased muscle tone may add stability to the weakened ligamentous structures. Conversely, a hypomobile SI joint may benefit from massage or other soft-tissue manipulation targeted to these particular muscles if they are restricting appropriate motion.
Piriformis to posterior sacroiliac ligament
Fascia covering the posterior aspect of the piriformis muscle is contiguous with the lower margins of the posterior sacroiliac ligament complex (Figure 3). The pull of the piriformis is such that it, too, contributes lateral compressive force to the SI joint.
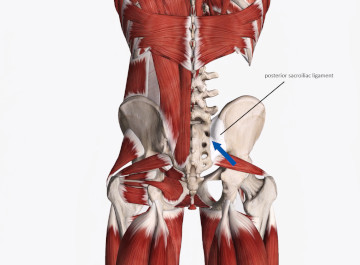
Figure 3
Fascia from posterior piriformis is contiguous with lower margins of posterior sacroiliac ligament complex
Image is from 3D4Medical’s Complete Anatomy application
The piriformis muscle is susceptible to hypertonicity, and consequently excessive tension on the muscle could be transmitted to the posterior sacroiliac ligaments. The lower posterior sacroiliac ligaments become taut during counternutation, so in this position it may put additional tensile stress on the piriformis muscle as well.
Tension on the piriformis may have other interesting ramifications for SI joint pathology. Pain that is felt in the gluteal region is often suspected to originate from piriformis syndrome (entrapment of the sciatic or other gluteal region nerves by the piriformis muscle). One of the common methods for evaluating the presence of piriformis syndrome is the side-lying piriformis test, also called the FAIR (Flexion, Adduction, Internal Rotation) test. In this test the piriformis is put in a stretched position to assess if irritation occurs, producing symptoms of nerve compression. However, SI joint dysfunction may also produce pain in the gluteal region.
When tension is placed on the piriformis muscle during the FAIR test, that tension may translate to the SI joint through the posterior sacroiliac ligaments and cause a positive test. In this situation the positive result is not indicative of nerve compression, but of SI joint dysfunction that reproduced its characteristic pain with tension on the piriformis muscle. This is an example of why it is so important not to rely on a single evaluation procedure (like the FAIR test), to evaluate complaints in this region. There should be a comprehensive evaluation where multiple evaluation methods point to a most likely result for the client’s symptoms.
Sacroiliac ligaments to erector spinae
There is a direct longitudinal connection between the posterior sacroiliac ligaments and the inferior erector spinae fibers (Figure 4). Due to the numerous muscular and ligamentous connections between the lumbar spine and the pelvis, these two regions are inextricably linked. Lumbar lordosis is a good example of how the combined forces from these different tissues impacts the SI joint.
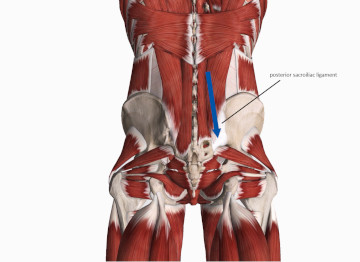
Figure 4
Posterior sacroiliac ligaments connect with inferior erector spinae fibers
Image is from 3D4Medical’s Complete Anatomy application
An exaggerated lumbar lordosis is usually produced by hypertonicity in the iliopsoas as well as the erector spinae. When the lordosis is increased it causes an anterior rotation of the pelvis, which then produces a relative posterior tipping (counternutation) of the sacrum.
The posterior sacroiliac ligaments are increasingly taut during counternutation. Therefore, when the erector spinae encourage the anterior pelvic tilt, not only do they pull on the sacroiliac ligaments through their fascial connections, but also increase tensile stress on these ligaments due to the increased counternutation at the SI joint. The additional tensile load on the ligaments may produce SI joint pain.
Finding ways to effectively treat SI joint pain is a continuous effort by practitioners from diverse professions. Clearly, the mechanics of this joint region are complex and multi-dimensional. The complexity of anatomical structures and biomechanical forces that govern the joint make accurate identification of SI joint pathology very challenging. The most effective treatments for SI joint dysfunction involve improving stability as well as soft-tissue manipulation and joint mobilization. Massage can play a fundamental role in this process, and the most effective approaches begin with a better understanding of the biomechanical function of this region.
- Vleeming A, Mooney V, Stoeckart R. Movement, Stability, & Lumbopelvic Pain. Edinburgh: Churchill Livingstone; 2007.