
There are numerous causes of anterior knee pain, some more common than others. Osteochondritis dissecans (OCD) is not a very common condition. It is, however, something that the massage practitioner should be aware of as a possible cause for knee pain. Osteochondritis dissecans is most often seen in younger patients, generally between 13 and 21 years old and is present in males more than females. Osteochondritis dissecans can occur in several regions of the body, but mainly in the knee, the capitellum of the elbow, and the talar dome of the foot. Our focus in this article is the knee.
PATHOLOGY
The tibia and femur are covered by a layer of hyaline cartilage on their ends that reduces friction and wear at the joint. In osteochondritis dissecans, a section of hyaline cartilage (and sometimes the underlying bone, called subchondral bone) separates from the remainder of the deeper bone. This separated fragment can float freely within the joint causing locking, pain, clicking, or crepitus during movement.
The name of the condition reflects earlier beliefs that it involved inflammation (thus the suffix ‘it is’). The current understanding is there is no significant inflammation associated with the cartilage and bone damage.1 Several authors have suggested that a more appropriate name for this condition would be osteochondrosis dissecans. The suffix –osis means abnormal condition, so this term would actually mean abnormal condition of the bone and cartilage instead of inflammation of the bone and cartilage.
It is the lateral side of the medial condyle of the femur that is affected usually in osteochondritis dissecans. Repetitive contact of the medial condyle against the tibial spine during various knee motions that causes irritation (Figure 1). The tibial spine is where the anterior cruciate ligament attaches to the tibia.
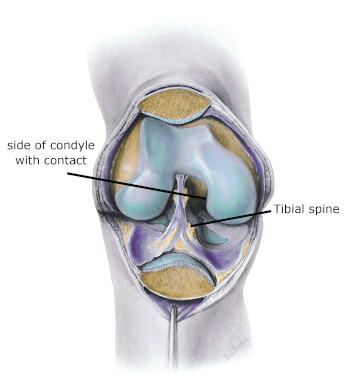
Figure 1
Primary region of contact
Mediclip image copyright (1998) Williams & Wilkins. All Rights Reserved.
It is unclear exactly how the process of cartilage degeneration and separation from the bone starts. There is some evidence that it occurs from previous trauma, repetitive impact loading, or abnormal ossification of the bone. In addition, it is thought that tensile forces of the cruciate ligament attachment may pull on the bone enough to weaken the osteochondral interface (Figure 2).
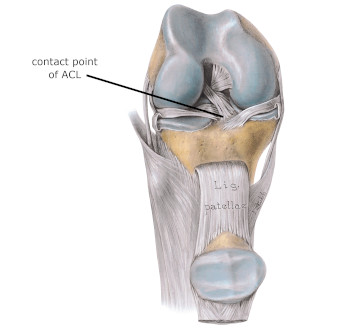
Figure 2
Knee in flexion showing attachment point of ACL
Mediclip image copyright (1998) Williams & Wilkins. All Rights Reserved.
Most likely it is due to multiple causes occurring at the same time. In some cases avascular necrosis may develop and precede the cartilage separation. Avascular necrosis is a process in which the blood supply to an area is decreased for some reason and the result is local tissue damage and tissue death (necrosis).
There is evidence that a discoid meniscus can contribute to the development of osteochondritis dissecans. A discoid meniscus refers to the shape of the meniscus of the knee. A normal medial meniscus is somewhat round when the individual is very young and then it opens up into a “C” shape as the person ages. A discoid meniscus maintains much more of its round or “O” shape, affecting the way the femoral condyle tracks with the meniscus. In cases, MRI investigations indicate evidence of meniscal damage in patients with osteochondritis dissecans.
ASSESSMENT
Osteochondritis dissecans in the knee is easy to mistake for other knee problems. X-ray or MRI are the most reliable tests for osteochondritis dissecans. There are other signs and symptoms however. With active or passive range of motion in the knee, clicking or crepitus may be evident with flexion or extension. Pain may occur along with the clicking movements if a loose piece of cartilage is floating in the knee. Pain is described as deep within the knee joint.
Thigh atrophy is another factor that is often used to identify knee pathology. As a result of joint dysfunction there is often some atrophy of the quadriceps muscles. Although a difference in thigh girth measurements does not specifically indicate osteochondritis dissecans, it is a common finding with this condition.
The Wilson test is valuable method for identifying osteochondritis dissecans that is affecting the medial condyle of the femur (Figure 3). In this procedure, the knee is extended while held in internal rotation. If pain is felt at around 300 of flexion, this could indicate a lesion on the medial condyle. The tibia is then moved into external rotation. If the pain is relieved with the external rotation, this is a positive test. This test can be performed both as an active movement and also with the knee being extended against resistance. If any internal joint clicking, crepitus, or group of signs and symptoms indicating possible osteochondritis dissecans exist, the individual is referred to a physician for further evaluation.

Figure 3
Position used for the Wilson test
Other knee complaints have similar symptoms and should also be considered. Meniscal tears, internal ligament sprains, and injury to the coronary ligaments that hold the menisci in place may produce pain felt deep in the joint similar to osteochondritis dissecans. Chondromalacia patellae may cause crepitus and grinding sensations. Patellar tracking disorders are also likely to cause quadriceps atrophy that show up with thigh girth discrepancies and diffuse anterior knee pain. Osteoarthritis may also have similar joint pain sensations.
TREATMENT
Most patients with this condition are young. Conservative treatment with this population is often effective because they are skeletally immature and can address the symptoms with activity modifications to reduce biomechanical stresses. With older patients, conservative treatment appears to be less effective and there is a greater likelihood that surgery will be necessary.
Conservative treatment often includes patellar taping and exercises for the vastus medialis obliquus muscle. The primary goal is to improve knee joint biomechanics, which decreases aggravation of the osteochondral lesion.
Surgical procedures for osteochondritis dissecans are primarily arthroscopic. That means there will be a minimal level of irritation and a quicker recovery. Chondroplasty is a procedure in which damaged cartilage is removed. However, in some cases there may still be pain and crepitus with movement. In addition once cartilage has been removed in an area, there is a greater chance that the individual will develop osteoarthritis later in life due to greater friction between the joint surfaces.
It is not clear whether massage is of significant benefit for this condition. However, there does not appear to be anything in the etiology of osteochondritis dissecans that suggests massage can be harmful or contraindicated as long as it is performed within comfort limits. Local and specific massage applications to the knee joint may prove beneficial in helping reduce corresponding soft-tissue pain in the region. It is still unclear if massage would have any benefit for aiding the restoration of adequate blood flow in the region. However, massage has general pain relief benefits outside of the specific condition treatment.
Time can be an important factor in getting good results from treatment. The longer joint microtrauma persists, the greater is the potential damage in the region. Clients exhibiting symptoms of osteochondritis dissecans should be referred to a physician as soon as possible so the condition can be appropriately evaluated and necessary treatment begun. As noted, massage is not contraindicated for this problem and may reduce associated pain from the articular damage.
Notes
- Grimm NL, Weiss JM, Kessler JI, Aoki SK. Osteochondritis dissecans of the knee: Pathoanatomy, epidemiology, and diagnosis. Clin Sports Med. 2014;33(2):181-188. doi:10.1016/j.csm.2013.11.006.