
A recent interesting case reveals how lateral hip and thigh pain can easily be misinterpreted and ascribed to other causes. A client, who I will call Steve, was experiencing lateral hip pain around the greater trochanter of the femur. Some pain was extending into the lateral thigh region as a deep aching sensation.
One practitioner thought that Steve had trigger points in his gluteus minimus muscle, and another thought he had a joint capsule problem. Treating the trigger points via direct pressure on the tissues gave some brief intermittent relief but ultimately was unsuccessful in resolving the issue. In this instance, an alternative explanation seemed necessary for Steve’s symptoms.
Lateral thigh and hip pain, often mistaken for other conditions, can stem from an overlooked cause: entrapment of the lateral femoral cutaneous nerve (LFCN), also known as meralgia paresthetica. This case underscores the necessity of considering LFCN entrapment as a potential cause of lateral hip and thigh pain.
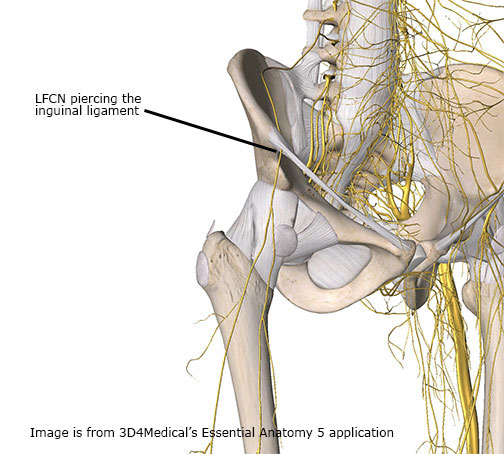
The LFCN originates from the L2 and L3 lumbar nerve roots and then courses around the inner aspect of the iliac crest. It then descends beneath the inguinal ligament. It takes a very sharp bend just as it passes the inguinal ligament, which is one of the locations where it is frequently entrapped (Figure 1).
The lateral femoral cutaneous nerve (LFCN) courses down the thigh, passing under the inguinal ligament and through a cylindrical band of connective tissue around the thigh called the fascia lata. This connective tissue can compress the nerve, especially when wearing tight clothing like jeans or restrictive gear. Compression can also occur in individuals with obesity or diabetes due to increased pressure on the nerve. Some people find pain sensations from LFCN compression so strong that they won’t put things in their pocket on that side because of additional pressure on the nerve.
Symptoms from LFCN compression can include pain, coldness, numbness, paresthesia, disturbances in sensation, or itching or buzzing sensations in the skin of the lateral hip or thigh. LFCN compression is often mistaken for conditions such as lumbar nerve root pathology, trochanteric bursitis, hip joint pain, joint capsule problems, abductor muscle pain, myofascial trigger points, or iliotibial band pain. It is common for manual therapy practitioners to engage direct treatment of these tissues in an effort to address the pain problem. However, in many cases this treatment approach might cause further aggravation of the problem if they do not recognize that the disorder is coming from nerve compression. Manual compression of nerves from soft-tissue work can further aggravate the condition.
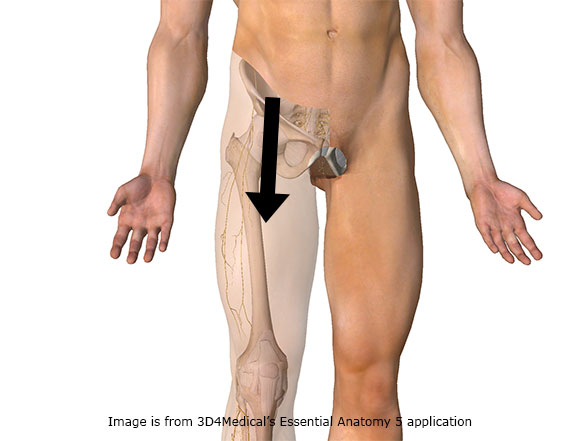
The LFCN is a very small nerve and often the region of compression is simply a small area where the nerve is constricted as it perforates through another tissue. One of the more effective ways to address this type of disorder is simply applying traction to the skin and pulling the skin over the upper anterior thigh in an inferior direction (Figure 2). This treatment actually helps to mobilize the nerve tissue and decrease the degree of binding between the nerve and adjacent tissues that it is interfacing with.
If you look at many of the current fitness magazines or advertisements that appear throughout social media, you will see frequent references to soft-tissue manipulation methods such as foam rollers, massage tools, or all kinds of other treatment methods to address pain throughout the iliotibial band and lateral thigh.
It is possible that LFCN entrapment is at the root of the problem and continuing to press on the structures further with foam rolling or deep manual therapy, may only serve to prolong the condition and exacerbate the problem. Yet the solution may be as simple as pulling the skin on a frequent basis to give appropriate mechanical relief to this nerve, which would then decrease irritation and eliminate the pain complaint.