
Joint motion is usually described as a movement between two articulating bones. That is an accurate description of joint mechanics at most skeletal joints in the body. Spinal motion however is more complicated, as it involves multiple joints. It also includes many soft-tissues spanning those joints. In this issue we look at the complexities of lumbar spinal structure and how it influences movement. We’ll also look at how dysfunctional mechanics may bring people into our treatment rooms. A key concept to understand with spinal motion is the motion segment, also sometimes called the functional unit of the spine. The motion segment includes two adjacent vertebrae and the intervertebral disc between them. The many soft tissues that span between adjacent vertebrae may also be considered part of the motion segment. We’ll explore all these tissues and their influence on spinal mechanics focusing on the lumbar region.
Structure of the Motion Segment
We can divide the motion segment into anterior and posterior components. Imagine a vertical line posterior to the vertebral bodies as the dividing line between the anterior and posterior elements (Image 1). The anterior components of the motion segment include the vertebral body, intervertebral disc, and the anterior longitudinal ligament.
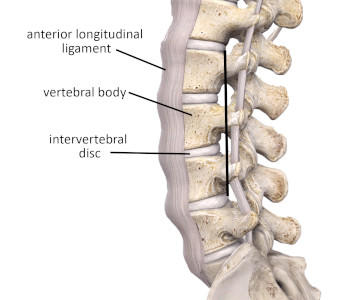
Image 1
Anterior components of the motion segment
Image is from 3D4Medical’s Complete Anatomy application
The intervertebral disc and vertebral bodies manage the large compressive loads of the spine. The majority of upper body weight is transmitted to the skeleton of the lower body through the lumbar spine. That is why the intervertebral discs and vertebral bodies are largest in the lumbar region. The lumbar motion segments must carry that compressive load while still being mobile. The third component, the anterior longitudinal ligament, limits spinal extension and helps maintain the structural integrity of the intervertebral disc.
The intervertebral disc is a shock-absorbing cushion between adjacent vertebrae. That is its primary role. It is composed of an inner gel-like substance called the nucleus pulposus, and is surrounded by a firm fibrocartilage container of concentric rings called the annulus fibrosus. The concentric rings of the annulus are oriented in alternating directions, which helps the annulus resist the high bending and torsion loads on the spine.
Where the vertebral body articulates with the disc there is a strong hyaline cartilage border called the vertebral end plate. There is no direct blood supply to the intervertebral disc. The disc relies on diffusion of its nutritional supply from the vertebral end plate. High compressive loads impair diffusion of nutrients to the disc and may be one of the factors leading to chronic disc degeneration from long-term loading.
The motion segment’s posterior portion includes the vertebral arches, the facet (zygapophyseal) joints between the adjacent vertebra, transverse and spinous processes of the vertebrae, and the supporting ligaments that span between adjacent vertebrae. The supporting ligaments include the intertransverse, interspinous, and posterior longitudinal ligaments. (Image 2). The primary role of the posterior motion segment is to guide and restrain spinal movement in specific directions.
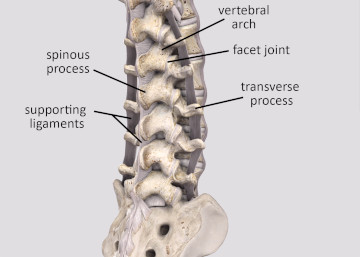
Image 2
Posterior components of the motion segment
Image is from 3D4Medical’s Complete Anatomy application
The main guide for lumbar spinal movement is the orientation of the facet joints. In the lumbar spine, the facet joints are mostly vertical, allowing the greatest range of motion in spinal flexion and extension. There is some degree of lateral flexion in the lumbar spine and a small amount of rotation. The majority of trunk rotation occurs in the thoracic region. There is minimal flexion and extension in the thoracic region due to the rib cage.
The supporting ligaments of the posterior motion segment contribute a great deal to its stability. The intertransverse ligaments span between each of the transverse processes. The interspinous ligaments span between each spinous process. These supporting ligaments act as guy wires to maintain vertical spinal stability. There is a constant balance between mobility and stability in the spine as we stand on two feet in the vertical gravity plane. Many soft tissue problems develop from dysfunctional mechanics in the lumbar motion segments. Next we’ll take a look at some key aspects of lumbar spinal mechanics for the motion segments.
Biomechanical factors
All spinal movements involve the coordinated action of adjacent motion segments. When movement is limited at one or more segments, mobility can be lost in those adjacent as well. As a result, coordinated spinal mechanics will suffer. For example, suppose a client has significant hypertonicity in the lumbar spinal extensors between L3 and L5 and corresponding low back pain. The hypertonicity will limit their ability to properly flex the lumbar spine when bending forward.
The limitation in spinal movement during forward flexion causes more anterior pelvic rotation as they attempt to bend forward. The altered mechanics also places increased tensile loads on the hamstrings due to the pelvic rotation, which can make them more susceptible to injury or dysfunction.
The facet joints of the spine are another region susceptible to altered motion segment mechanics. The facet joints have a minimal amount of loadbearing function in normal spinal mechanics. Yet, particular postural challenges, such as an exaggerated lumbar lordosis, shift the loadbearing vector to the posterior motion segment. When the weight shifts posteriorly, the facet joints must bear increased weight (Image 3). Carrying more weight makes the joints more susceptible to degenerative changes that may contribute to lumbar facet syndrome or arthritis.
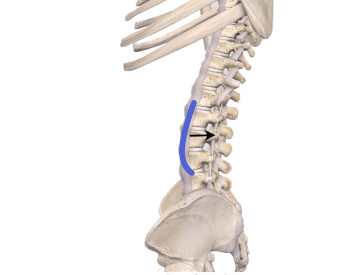
Image 3
Lumbar lordosis & the motion segment.
With increased lordosis (blue line) weight-bearing shifts posteriorly (black arrow)
Image is from 3D4Medical’s Complete Anatomy application
As noted earlier, the anterior structures of the motion segment are the primary ones bearing weight and transmitting compression loads through the spine. Long periods in poor posture combined with muscle tightness can increase compressive loads on the anterior motion segment components. Degenerative changes in the spine may result from these chronic compressive loads.
Another condition involving the motion segments is intervertebral disc pathology, which is often the result of prolonged mechanical loading in the lumbar spine. Excess compression causes the nucleus to push out into the annulus and deform the disc. This disc deformation is the condition known as a disc herniation (Image 4). These degenerative changes also shift greater weight-bearing responsibility to the posterior part of the motion segment. They may also lead to pain or other degenerative changes in the spinal structures.
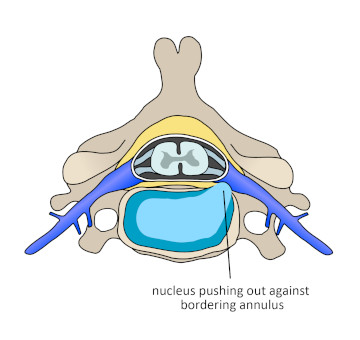
Image 4
Intervertebral disc herniation
Image courtesy of Wikimedia Commons
The intervertebral disc is actually quite resistant to compressive loads. It can take long periods of compressive loading without deformation. Studies have attempted to identify how much compressive load lumbar discs can manage before causing an acute herniation or rupture. Under high compressive loads, the vertebral endplates will often fracture before causing a disc herniation.
Another illustration of the importance of motion segment mechanics is the lumbar fusion surgery. Surgeons perform a fusion when there is a severe degree of disc degeneration and additional movement within the segment risks further damaging spinal structures. The surgery limits or stops motion altogether at one segment. The intention is to decrease the cumulative forces that contribute to spinal dysfunction. Yet, decreasing motion at one segment also decreases motion at segments above and below the fused segment. The resulting limited mobility in the soft tissues that span the segment means they can no longer move through a full range of motion, which makes them more prone to chronic hypertonicity and contribute to back pain. Massage can help these soft tissues stay in a more healthy and functional state and reduce back pain.
Implications for Massage
Normalizing muscular mechanics of the motion segment is a valuable goal of massage treatment. Hypertonic muscles that restrict ideal movement between adjacent motion segments are a root cause of back pain. Massage treatment excels at addressing this tightness, and helps increase mobility. Any treatment should start with general overall techniques that work to relax the region. After that, more specific treatments can be used to address a number of key muscles acting on the motion segment.
Numerous muscles in the lumbar region have a primary role in maintaining stability and producing movement in the motion segments. Interestingly, the latissimus dorsi is not one of them though it lies over the entire low back region. This muscle lies over the other muscles that might be treated in conditions involving movement challenges with the motion segments. Yet, massage of the latissimus is valuable to create general relaxation before working on deeper layers.
The next muscle layer we focus treatment on includes the three divisions of the the erector spinae group: spinalis, iliocostalis, and longissimus. Clients often have pain in this muscle group and massage can bring immediate improvement through pain reduction and increased mobility. These muscles are relatively superficial, so they are easy to address in treatment. Hypertonicity in the erector spinae group can produce significant reduction in range of motion and subsequent altered motion segment mechanics so they are an important group to treat. These muscles seem to respond best to treatments that work in a parallel direction to their fibers running along the spine.
Deep to the erector spinae are the multifidus and quadratus lumborum. The quadratus lumborum also impacts motion segment mechanics and plays a crucial role in spinal mobility, especially in lateral flexion movements. This muscle is best addressed by working lateral to the erector spinae group. Because it is farther away from the spine and not fully under the erector spinae muscles, it is a little easier to access than some of the deep intrinsic muscles along the spine (Image 5).
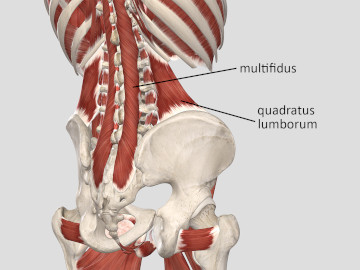
Image 5
Deep muscles controlling the lumbar motion segment
Image is from 3D4Medical’s Complete Anatomy application
Most of the multifidus is directly below the erector spinae, so it is not as easy to access. You can work the multifidus to some degree with pressure directly on the spinal extensors. You can also reach some portions of it by working with a small contact surface such as a thumb or fingertip directly in the lamina groove. The multifidus sometimes gets ingnored because people are apprehensive of working so close to the spine. As long as appropriate pressure is used along with good client communication, this is a safe area for massage.
Massage is often used in conjunction with spinal manipulative therapy. However, biomechanical analysis suggests that pain relief and enhanced movement from manipulations are most likely from improved motion segment mobility and not pushing vertebrae back into a particular position. Vertebrae are bound together with strong ligaments. In addition, the intervertebral discs having fibers embedded into the vertebral bodies above and below. Muscles also cross the joints of the motion segments to provide additional stability. As such, it is very difficult for one vertebra to be out of position in relation to those adjacent to it. Consequently, the understanding of spinal manipulative therapy has evolved to look at other mechanisms.
Low back pain is one of the primary reasons people seek the care of a massage therapist. So it is beneficial to understand key components of spinal mechanics. Even when clients have a more serious complication such as a herniated intervertebral disc, massage can help resolve hypertonicity, and restore optimal spinal mechanics and mobility. The more we understand about these functional relationships, the better we can employ appropriate strategies in the treatment room and with home care suggestions for our clients.