
The piriformis muscle is one of the six deep rotators of the hip and lies deep to the gluteal muscles (Figure 1). Even though it is small, the muscle plays a vital role in hip mechanics. Figure 1 shows the piriformis muscle in relation to the surrounding pelvis. Note that the muscle attaches to the anterior facet of the sacrum, crosses the sacroiliac and hip joints, and then attaches to the greater trochanter of the femur.
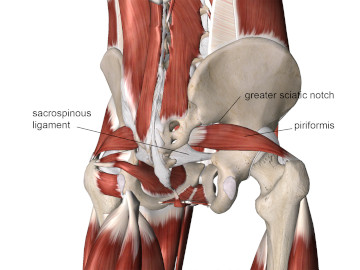
The image shows that the superior portion of the muscle passes very close to the greater sciatic notch. The small space above the piriformis muscle is called the supra-piriformis foramen, and this narrow space plays a key role in nerve compression. Just below the piriformis muscle is the sacrospinous ligament, which is a stiff and unyielding structure. It is also important in creating nerve compression problems in this region.
The piriformis muscle plays a key role in musculoskeletal conditions such as piriformis syndrome, in which the muscle compresses the sciatic nerve as it exits the greater sciatic foramen. There are other causes of piriformis syndrome, but most involve some degree of piriformis tightness. Piriformis syndrome is usually described as compression of the sciatic nerve by the piriformis muscle. While the sciatic nerve is the nerve most frequently involved, there are actually five different nerves that could be compressed in this condition.
The sciatic nerve has two primary divisions, and in some cases, one or both divisions may pass directly through the piriformis muscle. In this case, it’s easy to understand how hypertonicity in the piriformis muscle could squeeze the sciatic nerve and cause radiating neurological symptoms. In other cases, hypertonicity in the piriformis compresses the sciatic nerve against an adjacent structure, such as the sacrospinous ligament. Myofascial trigger points are also likely to be present when the hypertonic piriformis is causing these complications.
Hypertonicity in the piriformis and other hip rotators can be observed during gait patterns with what is commonly referred to as foot turnout, in which the distal end of the foot points laterally. Turnout is easy to observe if the person is walking on a beach or in the snow, where footprints can be left. A slight degree of turnout is normal and should not be considered pathological. However, excessive turnout is commonly indicative of shortness or tightness in the piriformis muscle. Ballet dancers are prone to this condition as they employ turnout in their dance positions; constant contraction can lead to chronic overuse conditions.
Muscular hypertonicity is frequently treated with various compression and deep longitudinal stripping treatments. However, the piriformis lies deep to the large gluteus maximus, so it is harder to deliver specific treatment to the deeper piriformis muscle. In addition, direct pressure, whether by static compression or deep stripping methods, could further irritate the existing nerve compression.
For this reason, stretching is often used to address the tight piriformis because it is less likely to have contraindicated outcomes. There is a unique feature of the piriformis muscle that may cause certain common piriformis stretching positions to seem counterintuitive. The piriformis is attached to the anterior face of the sacrum proximally and to the upper regions of the greater trochanter of the femur distally (Figure 1). Its primary action is lateral rotation of the femur, although it contributes to other actions as well. For example, when the thigh is flexed to 90 degrees the piriformis is a more prominent hip abductor.
The piriformis muscle is similar to several other muscles in the body in that it may change its primary action depending on the relative position of the joint(s) it crosses. Let’s take a look at how this works in the piriformis.
Notice the distal attachment of the piriformis tendon across the top side of the greater trochanter of the femur in Figure 1. Also, notice that the greater trochanter of the femur is ‘pointing’ upwards. Viewing the greater trochanter from above, the piriformis attachment is slightly in front of (anterior) to the axis of rotation for the femur. Certain tendon fibers also wrap around the trochanter from the back side. Therefore, if the hip is in a neutral position when the piriformis contracts, it pulls along the back side of the trochanter and forces the femur to rotate laterally as the front side of the femur is pulled laterally.
However, the piriformis’ main action changes significantly when the hip is in about 60 degrees or more of flexion. In this position, the upper margin of the greater trochanter ‘points’ in a downward direction, changing the piriformis’ action. With the hip flexed, the piriformis pulls the femur in medial rotation instead of lateral. Once you are past 60 degrees of hip flexion, the piriformis becomes a medial rotator and a prominent hip abductor.
The position shown in Figure 2 is commonly used to stretch the piriformis (the image shows a left-side piriformis stretch). If you perform this stretch on yourself, you can probably feel the deep sensation of stretching as you pull the hip closer to your chest. However, note that the left hip is laterally rotated in this position. If the piriformis maintains its primary action of lateral rotation when the hip is in a neutral position, this would not stretch the muscle; rather, it would shorten it.

Understanding the biomechanical forces at play in various stretching positions is very helpful for knowing how to target a specific muscle for stretching. Understanding the complexities of hip joint mechanics will help you develop optimum treatment and home care suggestions that will be most effective for your clients.