
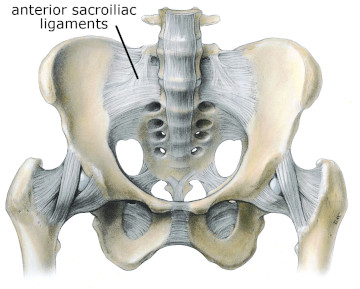
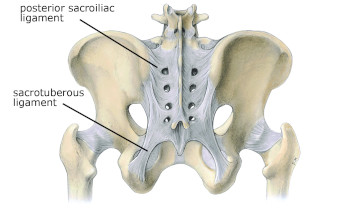
The sacroiliac (SI) joint is one of the most biomechanically complex joints in the body. Yet there is actually very little movement in the joint because of its need for stability. The SI joints are tightly bound with a dense webbing of ligaments on both the anterior and posterior sides. The primary stabilizing ligaments are the anterior sacroiliac, posterior sacroiliac, sacrotuberous, and sacrospinous ligaments (Figures 1 & 2). In this issue we’ll take an in-depth look at one of the most important supporting ligaments in this region, the sacrotuberous ligament.
Anatomical & Biomechanical Considerations
The sacrotuberous ligament connects the sacrum to the ischial tuberosity of the pelvis. On its proximal end its fibers blend with those of the posterior sacroiliac ligament and the sacroiliac joint capsule. Distal fibers of the multifidi and erector spinae also mesh with the proximal fibers of the sacrotuberous ligament.
On its distal end sacrotuberous ligament fibers are contiguous with those of the proximal hamstring attachment at the ischial tuberosity. In particular, fibers of the biceps femoris frequently extend beyond the ischial tuberosity to join directly with the sacrotuberous ligament.
The fascial connection between the hamstrings and the sacrotuberous ligament has important implications for SI joint function. There is a slight degree of motion at the SI joint where the sacrum moves back and forth in the sagittal plane. The forward tipping of the superior surface of the sacrum is called nutation and the backward tipping is called counternutation. The range for both is only about 7–8 degrees.
This motion is essential for proper mechanics during walking, bending over, and other motions because each half of the pelvis must move slightly independent of the other. The sacrotuberous ligament is attached to the lower margin of the sacrum so it becomes taut during nutation and somewhat slackened during counternutation.
The hamstrings and sacrotuberous ligament work in conjunction with each other for proper SI joint mechanics. Another way to view this connection is by imagining what occurs when the hamstring muscles are too tight. Tight hamstrings can cause the innominate (ilium, ischium, & pubis on one side) to rotate posteriorly. As the innominate rotates posteriorly there is a relative nutation at the SI joint, putting increased tension on the sacrotuberous ligament. Consequently, there is greater tension on the sacrotuberous ligament both from resisting the nutation as well as the fascial connections pulling on it from the tight hamstrings. Working on tension reduction in the hamstrings could therefore be an important factor in some conditions of SI joint dysfunction.
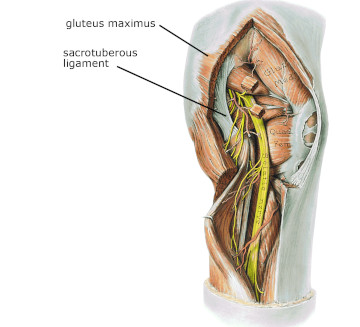
The hamstrings are not the only muscle group that has fascial connections to the sacrotuberous ligament. The gluteus maximus also has fascial continuity with the ligament (Figure 3). It is the largest muscle in the body and consequently is capable of generating very large force loads. Because of its strong pull, it can also exert tension on the sacrotuberous ligament and affect mechanics at the SI joint.
Clinical Applications
The connective tissue links between muscles and the sacrotuberous ligament are important to consider during assessment. For example, a client might present with pain down the posterior lower extremity. That pain could originate from a neurological disorder, but SI joint dysfunction can also produce a similar pain pattern.
The straight leg raise test is commonly used to evaluate neurological disorders and the client may report pain reproduction during the test. However, pain may be reproduced because the hamstrings are pulling on the sacrum through the sacrotuberous ligament, causing irritation of the SI joint. Consequently a more thorough evaluation of nerve involvement vs. joint dysfunction is needed.
Stresses on these fascial connections don’t have to be large forces in order to have an impact. Due to the rich innervation of this area, even minor loads of tensile stress may be sufficient to cause irritation of the sensory receptors and produce significant back or SI joint pain. The sacrotuberous ligament is involved in numerous pelvic conditions so it only seems natural to attempt treatment of the ligament. However, we must remember the physiology of ligaments when attempting to treat them.
It is not uncommon to hear descriptions of “releasing” the sacrotuberous ligament through direct pressure, stripping, friction, or an assortment of other methods. Keep in mind that the sacrotuberous ligament is an inert tissue and does not have any contractile properties. Because it cannot contract, it also does not “release” when work is done in this area. It is far more likely that any sense of decreased tissue restriction or increased movement result from work on the muscles in the region. Due to the depth of the sacrotuberous ligament, when pressure is applied to the ligament you push on fibers of adjacent muscles so they are clearly being treated as well.
Finding ways to effectively treat lumbopelvic joint pain is a continuous effort by practitioners from diverse professions. Accurate assessment and effective treatment both rely on a solid understanding of the multiple tissues in this region. The sacrotuberous ligament is an important link in the kinetic chain through this area so its structure, function, and mechanical links need to be considered for accurate evaluation and treatment.