
The majority of ankle injuries involve sprains to the supporting ligaments of the ankle. Most occur to the ligaments on the lateral side of the ankle and are generally referred to as inversion ankle sprains because it is excessive inversion that causes the sprain. There are two other ankle regions that are also susceptible to ligamentous sprain: the deltoid ligament complex on the medial side of the ankle and the distal tibiofibular syndesmosis above the ankle joint. Let’s examine some key factors associated with each of these injuries.
Lateral Ankle:
Inversion ankle sprains affecting the lateral ligaments are often considered the most common lower extremity soft-tissue injury. The architecture of the leg and foot bones as well as the smaller size of these ligaments make them more vulnerable to injury. The primary function of the lateral ankle ligaments is to resist excessive inversion of the ankle. Yet for this important role, these ligaments aren’t as strong and resilient as those on the opposite side of the ankle. That is one of the reasons that inversion sprains are much more frequent than eversion sprains.
There are three primary ligaments that make up the lateral ankle ligament complex. Their attachment points are easy to identify as the ligament names designate the two bones they connect. These three key ligaments are the anterior talofibular (connecting the talus and fibula), posterior talofibular (also connecting talus and fibula), and the calcaneal fibular (connecting the calacaneus and fibula). Of these, the anterior talofibular and calcaneofibular are the most commonly injured with the inversion ankle sprain (Figure 1).
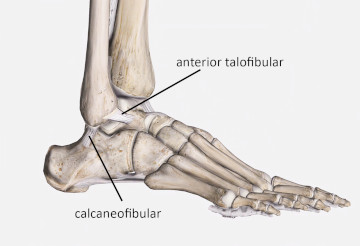
Figure 1
Anterior talofibular and calcaneofibular ligaments of the lateral ankle
Image is from 3D4Medical’s Complete Anatomy application
Excessive inversion is the most likely foot movement that sprains these ligaments. However extreme plantar flexion, especially if combined with inversion, is also a likely contributor to inversion ankle sprain. A common example of lateral ankle sprain is stepping off an elevated surface like a curb, or stepping down into a hole where the foot is both plantar flexed and inverted.
Alignment of the foot and ankle complex is essential to transmit body weight and ground reaction force through the foot and ankle region. Once the foot turns inward, it is no longer a stable base of support and the entire body weight magnifies the force these ligaments have to resist.
When a person has sustained an inversion ankle sprain, the primary goal is to prevent any excessive movement during the ligament’s healing so scar tissue can knit the torn fibers back together and maintain as much stability as possible. Deep friction techniques are often advocated to treat an ankle sprain, with the theory being that it can help reduce fibrous scar tissue that might adhere the healing ligament to adjacent soft-tissue. There has also been some speculation that friction massage may aid in fibroblast proliferation to help repair damaged tissue.
Medial Ankle (Deltoid Complex)
On the opposite side of the ankle is the deltoid ligament complex. It is sometimes just call the deltoid ligament, but it is actually a group of four separate ligaments. The name deltoid refers to the fact that as a group these ligaments make up a triangular shape, which is the Greek letter Delta.
The four separate ligaments that make up the deltoid group are the anterior tibiotalar, tibiocalcaneal, posterior tibiotalar, and tibionavicular (Figure 2). Similar to the lateral ankle ligaments, the names of these ligaments indicate which two bones they connect.
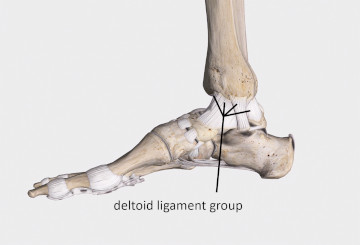
Figure 2
Four ligaments of the deltoid group on the medial ankle
Image is from 3D4Medical’s Complete Anatomy application
A sprain to the deltoid ligament complex is also referred to as an eversion ankle sprain because it is excessive eversion that causes the injury. There are two main reasons why eversion ankle sprains are less common than inversion sprains. First, the deltoid ligament group is much stronger than the lateral ankle ligaments. Second, the fibula extends farther distally on the lateral side of the ankle than the tibia does on the medial side. Because of this further extension, the fibula blocks the foot from moving to that side during eversion movements and consequently generates greater ankle stability against excessive eversion.
If the deltoid group has been stressed to the point of ligament injury, there were most likely excessive forces to the ankle to produce that injury. As a result, there are frequently other structural injuries that occur along with deltoid ligament sprains, such as fracture or dislocation. If your client sustained an injury sufficient to damage the deltoid ligament group, it is a good idea to have them evaluated by another health professional to make sure there aren’t other serious injuries along with the ligament damage.
Syndesmosis
A third group of ligaments are sometimes injured in what is called a high ankle sprain and involve connective tissues that are superior to the ankle. These injuries involve the syndesmotic ligaments that bind the distal tibia and fibula together. The webbing of connective tissue that binds the distal connection of the two leg bones includes the anterior inferior tibiofibular ligament, the distal posterior tibiofibular ligament, interosseous ligament, and the interosseous membrane (Figure 3).
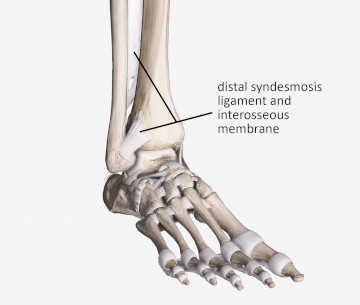
Figure 3
Distal syndesmosis ligament and interosseous membrane
Image is from 3D4Medical’s Complete Anatomy application
It is not that important to memorize these individual ligament names. The most important characteristic to remember is there’s just a tight webbing of ligamentous tissue binding the ends of the tibia and fibula. In addition, the joint is also bound by the interosseous membrane which spans between the tibia and fibula throughout the lower leg.
Injuries to the ankle syndesmosis are most likely to result from excessive rotation of the ankle (adduction or abduction of the foot), extremes of dorsiflexion, or combinations of dorsiflexion with adduction or abduction. In some cases the shearing and twisting forces applied to the ankle not only damage the distal syndesmosis ligaments, but can transfer through the interosseous membrane of the leg and cause damage much higher up than the ankle.
The type of injury that produces syndesmosis sprain commonly occurs in sports played on turf with cleated shoes. For example, suppose an athlete has a cleated shoe that digs into the turf and keeps the ankle relatively immobile. If that person falls forward (causing dorsiflexion of the foot) at the same time that s/he is attempting to turn to the side (causing rotational stress in the ankle), injury to the syndesmosis is likely.
The common lateral ankle ligament injuries are usually not difficult to identify because the injured ligaments are superficial, making their palpation much easier. However, in the syndesmosis joint, palpation of the injured ligaments is not easy because other soft tissues obscure the ligaments.
Unlike the medial and lateral ankle ligaments, the syndesmosis ligaments are not as easily palpated, and are also not as easily treated with soft-tissue therapy. The toe extensor and foot dorsiflexor tendons lie superficial to the distal syndesmosis, so any pressure in this area has to work through those tissues first.
It is valuable to have a good understanding of ankle mechanics and location for these different ligaments structures. Recognizing the forces required to cause certain types of injury can help pinpoint the type of tissue involved and allow us to direct our treatments most appropriately.