
The physical examination component of a comprehensive assessment includes the application of crucial knowledge and skills for the massage therapist. Performing these skills and analyzing the results form a critical core of the practitioner’s success in treating pain and injury conditions. Accurate assessment provides a foundational understanding of the client’s current condition and is the driver of treatment decisions. There are numerous methods of musculoskeletal assessment. Yet, one thing they all share is the recognition of biomechanical forces that may be the source of specific pain complaints. The application and analysis of mechanical forces within assessment strategies is what makes up assessment biomechanics.
The term biomechanics as it applies to musculoskeletal function is often misunderstood or used inaccurately. Biomechanics is the study of mechanical forces applied to biological systems. There are five types of biomechanical force that soft-tissues are subject to: compression, tension, torsion, bending, and shear. The majority of biomechanical tissue injuries result from just two of these – compression (when two structures are pressed together) and tension (when tissue between two contact points is pulled in opposite directions). Consequently, biomechanical assessment strategies focus primarily on compression and tension forces as well.
Applied anatomy is another essential component of assessment biomechanics. A key goal of the assessment process is to identify specific tissues that are likely involved in the client’s current pain complaint. Recognizing what happens to specific tissues during various movements or positions and under different movement conditions (active, passive, or resisted) helps identify when those tissues may be at the root of a particular pain complaint. An enhanced understanding of musculoskeletal anatomy is essential to accurately apply these concepts in the assessment process.
The standard assessment procedure used as the basis for this discussion of assessment biomechanics is the HOPRS procedure outlined in the text, Orthopedic Assessment in Massage Therapy. HOPRS is an acronym which stands for History, Observation, Palpation, Range of motion and resistance testing, and Special orthopedic tests. This discussion of assessment biomechanics focuses on the R portion (range-of-motion and resistance testing) of the HOPRS model. Interpreting results from the range of motion and resistance testing is the most important aspect of the physical examination for determining likely tissues involved.
The results from the range-of-motion and resistance testing help evaluate compression and tension forces various tissues are subjected to during those movements. If a specific movement reproduces the client’s primary pain complaint, there is a good chance the tissues being stressed (with compression or tension) during that movement are involved. The practitioner then cross references movements in that region to see if a pattern of results emerges that would further implicate or exclude a particular tissue(s).
There are five different evaluation scenarios where the compression and tension forces on various soft tissues are analyzed.
- Active Shortening: During active movement specific tissues may shorten or have existing tension forces reduced.
- Active Lengthening: In some active movements tissues will lengthen or have an increased tensile load when a limb or body region is actively moved.
- Passive Shortening: Tissues may shorten or have their tensile load decreased when a limb or body region is moved passively.
- Passive Lengthening: When body regions are passively moved, tensile forces may increase as tissues are pulled.
- Isometric (Manual) Resistance: Isometric contractions involve force generated by the muscle that pulls on the tendon, but no movement of the associated bones occurs. In assessment, the resisted actions show up during manual resistive tests. Muscle and tendon are the only tissues with significant forces on them during resisted actions.
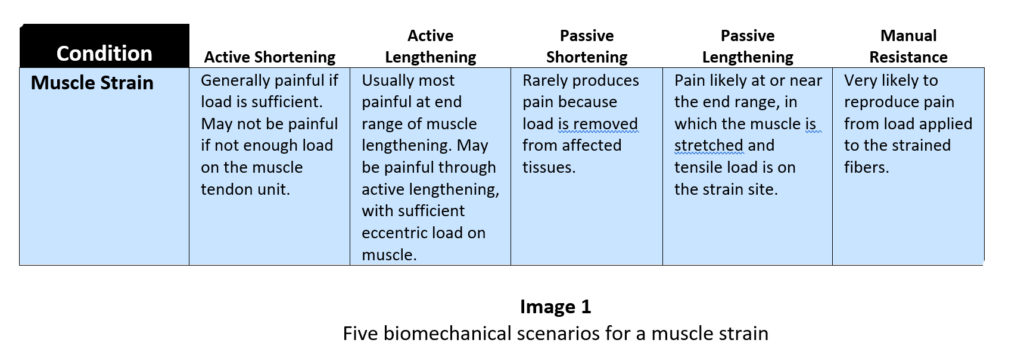
Certain musculoskeletal conditions (mainly those involving some degree of mechanical tissue insult or injury) produce common patterns during these five evaluation situations mentioned above. Recognizing the specific pattern of pain reproduction or pain relief can help clarify the presence or absence of various pathologies. For example, a muscle strain will have a particular pattern of results for each of the five evaluation procedures. If a muscle strain is suspected during the evaluation, the practitioner can determine if the various movements that produce or don’t produce pain fit the pattern. An easy way to evaluate these patterns is to look at them in a chart, such as the one illustrated in Image 1.
Let’s take a look at what happens in each of those five scenarios.
- Active Shortening: In a strain, muscle fibers have been overstretched or torn. When there is an active shortening contraction of the target muscle, the site of injury is pulled and pain is generally reproduced. Sometimes when you have a large muscle or a movement that does not require a high force load, a strain will not be painful with active movement unless there is additional resistance. For example, a strain of the gastrocnemius may not be painful if the client is sitting on the edge of the table and simply moving their foot in the air (active non-weight-bearing plantar flexion). Even though the muscle is being engaged there is not a high load demand on the involved muscle. Without a significant contraction force, not enough fibers are recruited to reproduce the pain of the muscle strain.
- Active Lengthening: With a muscle strain, the fibers of the muscle are pulled during active lengthening. The tensile load will be greatest near the end range when the muscle is getting fully stretched. Eccentric loads usually produce enough tensile force on the muscle to reproduce pain with a muscle strain, and pain will likely increase as the muscle further lengthens.
- Passive Shortening: During passive shortening there is no load on the muscle and any tensile forces decrease as the muscle length reduces. For that reason, pain decreases as the strained muscle further shortens if the movement is passive.
- Passive Lengthening: Similar to active lengthening, pain is likely to increase as the muscle is further stretched. There is no eccentric load on the muscle since the movement is passive, so pain is usually less than with active lengthening, but pain is still likely as the muscle length increases. Pain generally increases near the end range of available movement. The available range of motion may be significantly less than normal due to pain limiting the motion.
- Manual Resistance: Manual resistance puts an increased load on the affected muscle and is likely to reproduce pain if a muscle strain is present.
* A full copy of this evaluation framework (which we call the assessment cheat sheet) with references to muscle, tendon, ligament, nerve, cartilage and bursa injuries can be downloaded for free at: www.academyofclinicalmassage.com
Thinking about various soft-tissue injuries in categories like this helps manage and organize the load of information you may gather during the assessment process. I have found repeatedly over the years when teaching assessment that while most people learned how to perform range-of-motion evaluations in their basic training, they really didn’t get a firm grasp of how to interpret the information derived from those procedures. This visual representation helps make sense of all the information and organize it so you can use it effectively.
The framework presented above with the five different evaluation scenarios is helpful for confirming the involvement of specific tissues, or type of tissue when you already have an idea of the tissues at play. However when performing musculoskeletal assessment, you rarely know what type of pain or injury complaint you are dealing with at the outset. In that case, another framework can be used to help gather information about what might be causing your client’s existing pain complaint.
This next evaluation framework is far more detailed and really helps the practitioner consider multiple causes of pain or discomfort when performing the client evaluation. Each row of this comprehensive evaluation framework will look at:
- One particular joint region
- One motion at a time (ex. flexion, extension, abduction, etc.)
- One type of motion at a time (active, passive, or resisted)
- Which specific tissues are exposed to either compressive or tensile loads in the above scenario
Let’s see what that would look like for a client with anterior knee pain. During the physical examination process we will explore several knee movements to evaluate if they reproduce the client’s pain. Here’s what one of those movement patterns would look like if we plug it into this evaluation framework. The framework shows which tissues are subjected to compressive or tensile stress during active knee flexion. In active knee flexion we are looking at:
- Knee (joint region)
- Flexion (specific motion being tested)
- Active movement (type of motion).
The evaluation results are shown in the chart in Image 2.
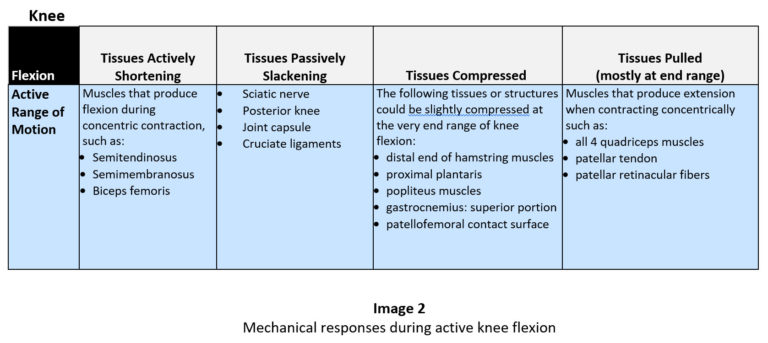
Now we have an idea of the various biomechanical stresses on several specific tissues during active knee flexion. This information will help us consider if any of those tissues might be contributing to our client’s current complaint. Having some knowledge of potential causes of knee pain in various motions will help us consider if any of these patterns seem likely for our client.
We can take this evaluation one step further by using another visual reference that shows several possible causes of pain in a particular region, with a particular motion, when it is performed either actively, passively, or resisted. Sticking with our previous example of active knee flexion here’s what that might look like.
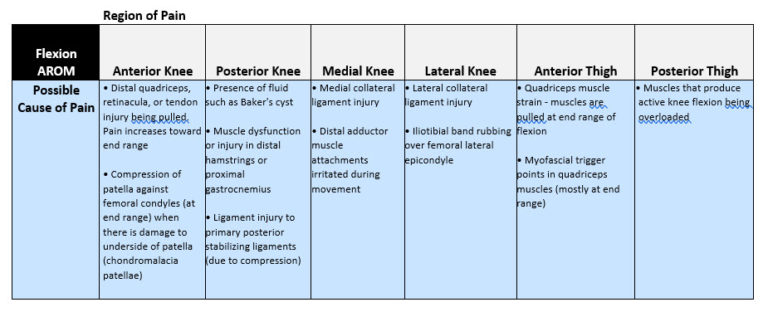
Our client was complaining of anterior knee pain, so we will be most interested in the findings in the first column listed under “Anterior Knee” as the region of pain. In this column there are two primary factors we see that are likely to cause anterior knee pain during active flexion. The distal quadriceps retinacula and patellar tendon are being pulled, especially near the end range. In addition there are compression forces on the underside of the patella that may also be a primary factor. Now that we have this information we can cross reference it with findings from other aspects of the assessment process and increase our accuracy in identifying tissues involved in the client’s complaint.
Applying this system of assessment biomechanics can streamline your assessment process and make your evaluation much more efficient. It also produces a much better understanding of particular tissues involved in your client’s condition, so you can choose the most effective treatment strategies. There is also an important underlying factor of this type of detailed assessment which is often underappreciated. Performing a detailed physical examination like this can boost your client’s confidence in your skills, and that increased client confidence greatly contributes to your treatment success.