
Introduction
Cultural colloquialisms develop from real world experiences. When something is very difficult or annoying we characteristically refer to it as a real “pain in the butt”. And, well that is the perfect description for this syndrome.
Sciatica is a poorly defined condition that generally refers to any pain sensation felt in the gluteal region or down the lower extremity along the path of the sciatic nerve. Many of these gluteal pain cases are caused by dysfunction of the piriformis muscle, a crucial deep rotator of the hip. Although there is no clear cut definition, the term piriformis syndrome describes gluteal pain involving the piriformis and compression of nearby nerve and vascular structures in the pelvis.
Sciatica (sciatic nerve compression symptoms) is usually ascribed to dysfunctions in the lumbar spine such as herniated discs or other causes of nerve root compression. However sciatica-like symptoms may also originate from the piriformis region. One study suggests that 5-6% of sciatica cases could likely involve piriformis syndrome, making it close to 2.4 million cases of the condition per year.1
With something that occurs so often it would seem likely that we’d have a very clear understanding of the condition, but that’s not the case. The concept of piriformis syndrome and entrapment of neurological structures in the pelvic region is still somewhat controversial. In fact, some medical professionals don’t even believe the condition exists.2 However, there is strong evidence to suggest that not only does this condition exist, but it is often under-recognized as a cause of gluteal and lower extremity pain and dysfunction. So let’s take a deep dive into this subject and see what is really going on.
Anatomy
Image 1 shows the piriformis muscle in relation to the surrounding pelvis. Note that the muscle attaches to the anterior facet of the sacrum, crosses the sacroiliac joint, crosses the hip joint, and then eventually attaches to the greater trochanter of the femur. Because it crosses both joints, there are biomechanical challenges that play a part in the condition.
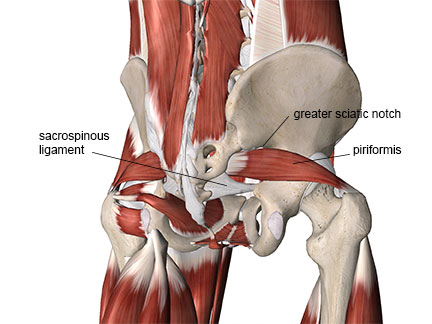
You can see in Image 1 that the superior portion of the muscle passes very close to the greater sciatic notch. The small space above the piriformis muscle is called the supra-piriformis foramen and this narrow space plays a key role in nerve compression, as we will see shortly. Just below the piriformis muscle is the sacrospinous ligament, which is a stiff and unyielding structure. It is also important in creating nerve compression problems in this region.
Piriformis syndrome is usually described as compression of the sciatic nerve by the piriformis muscle. While the sciatic nerve is the nerve most frequently involved, there are actually five different nerves that could be compressed in this condition. Let’s take a look at these various nerves and the regions where they are susceptible to compression.
In Image 2 you see that the superior gluteal nerve courses through the narrow opening of the supra-piriformis foramen. The superior gluteal nerve is primarily a motor nerve that supplies the gluteus medius and gluteus minimus muscles. When the piriformis is hypertonic, it can trap the superior gluteal nerve against the underside of the greater sciatic notch.
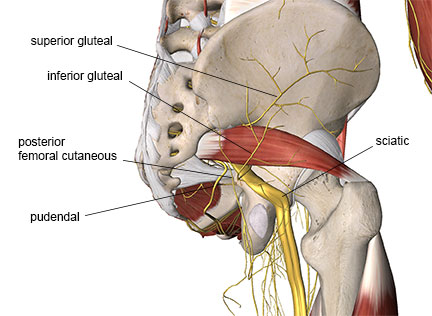
Next we’ll take a look at the infra-piriformis foramen and the four nerves that can be compressed by the piriformis there: sciatic, inferior gluteal, posterior femoral cutaneous, and pudendal. These nerves pass through the infra-piriformis foramen and are susceptible to compression between the piriformis muscle and the sacrospinous ligament.
If there’s one nerve in the body that most people are familiar with, it’s the sciatic nerve. It is the largest in diameter and longest nerve in the body. The sciatic nerve is composed of two divisions: the peroneal (or fibular) division and the tibial division. These divisions eventually split when the nerve passes around the posterior aspect of the knee. However, in some people they also split in the piriformis region and this can play a part in nerve compression.
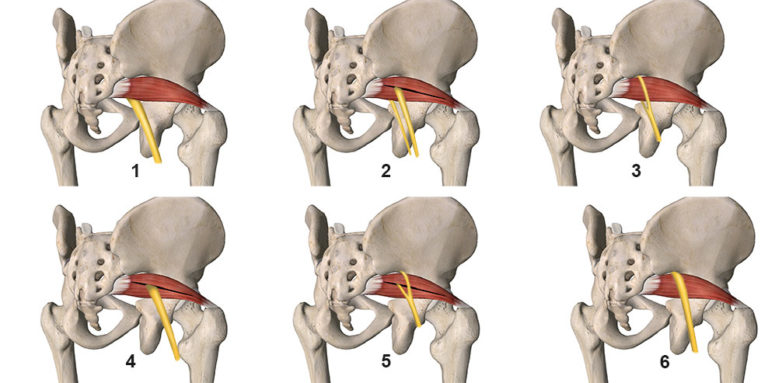
There are six anatomical variations that may occur between the sciatic nerve and the piriformis muscle.1 Image 3 shows these different variations.
Normal pathway of the sciatic nerve: The two divisions of the sciatic nerve remain together and pass inferior to the piriformis muscle. Both divisions course through the infra-piriformis foramen.
Peroneal division through the piriformis, tibial division below: In this variation the peroneal division passes directly through the middle of the piriformis muscle, while the tibial division is in the normal position. Nerve compression can be increased on the peroneal division by tendinous bands running through the muscle in addition to muscular fibers compressing the nerve.
Peroneal division above, tibial division below: Here the peroneal and tibial divisions are quite separated. The peroneal division courses through the supra-piriformis foramen above the muscle with the superior gluteal nerve, while the tibial division is in the normal position below the piriformis.
Both divisions through the middle of the muscle: Here both divisions course directly through the middle of the muscle. As with variation #2, tendinous bands within the piriformis muscle can further aggravate the nerve beyond the compression of the nerve fibers by the surrounding muscle.
Peroneal division above, tibial division through the muscle: In this variation the tibial division courses through the middle of the muscle while the peroneal division passes through the supra-piriformis foramen.
Both divisions above the muscle: The final variation is one in which both nerve divisions are above the piriformis and course through the supra-piriformis foramen. With both divisions of the muscle in the supra-piriformis foramen, there is less space for the superior gluteal nerve as well.
While sciatic nerve compression by the piriformis gets the most attention, the other nerves in this region shouldn’t be ignored. Running right next to the piriformis is the posterior femoral cutaneous nerve. As its name suggests it is primarily a sensory nerve supplying the posterior aspect of the thigh. Sometimes clients report posterior thigh neurological pain that only extends to the knee and not below it. In this case it is likely that the posterior femoral cutaneous nerve is being compressed.
The inferior gluteal nerve is a motor nerve that supplies the gluteus maximus. Because it is a motor nerve, compression of this nerve doesn’t cause as much pain but instead weakness or atrophy.
The last nerve susceptible to compression in this region is the pudenal nerve. It is rarely discussed in the literature about piriformis syndrome and is least often involved. However, it should not be ignored because nerve compression symptoms from this muscle could easily be ascribed to some other cause. The pudendal nerve is a mixed motor and sensory nerve. It innervates many of the pelvic floor muscles and supplies sensation to the perineal region, genitalia, and anus. Pudendal nerve compression also occurs from external factors such as very hard bicycle seats that can affect competitive cyclists that are racing for long periods.
Pathophysiology and Etiology
The piriformis muscle is primarily a lateral rotator of the hip. However, due to its attachment site, its action can change depending on the position of the hip. This also means the position to stretch the muscle taut can change along with hip position as well. When the hip is in a neutral position, the piriformis is a lateral rotator of the hip. However, once the hip flexes past about 600 it becomes primarily a hip abductor (from the flexed position) and can also contribute to internal rotation, thereby reversing its original action (Image 4).
Based on these biomechanical factors the piriformis is going to be stretched significantly when the hip is flexed or the person is sitting cross-legged. That is one reason piriformis syndrome occurs for people who sit for long periods.

Repeated loading of the piriformis in various activities has also been implicated as a cause for the condition. The piriformis can get stressed from repeated loads applied across the sacroiliac and hip joints, such as those that occur from running. In a situation like this the nerve compression may result more from chronic overuse of the muscle as opposed to other situations where external compression also plays a factor. Myofascial trigger points are also commonly present along with the nerve compression. One author noted that myofascial pain in the buttock region was present in 97% of the cases of piriformis syndrome they evaluated.1
Most often nerve pain is felt in the region of skin where the affected nerves supply cutaneous innervation. The nerves that are compressed in piriformis syndrome supply the posterior thigh and distal aspects of the lower extremity, but not the gluteal region specifically.
There are very small nerve fibers called nervi nervorum that innervate the nerves, and actually give sensory supply to the nerve fibers themselves. So these are the ‘nerves of the nerves’. It is likely that at least some of the pain in the gluteal region felt from nerves that supply the distal lower extremity may be from the nervi nervorum (small nerves that are giving sensory innervation to the sciatic and other nerves in this region).
Assessment
A detailed history and physical examination can help pinpoint which of the different nerves may be most involved in the condition. Keep in mind that you could have more than one nerve being compressed imaat the same time, but here are the key signs and symptoms to look for:
Superior gluteal nerve- Characteristic nerve symptoms of pain, paresthesia, or numbness will be mostly absent. Instead look for weakness in the hip abductor muscles (gluteus medius and minimus) as these are the muscles innervated by the superior gluteal nerve. Atrophy may be apparent in this muscle but sometimes weakness will be more obvious by comparing a test of resisted hip abduction on the affected side with that of the unaffected side.
Sciatic nerve: Gluteal pain is likely, but more frequently there will be shooting or radiating electrical-type pain that will extend down the lower extremity possibly all the way to the foot. Motor weakness is not as common with the sciatic nerve compression but can occur.
Posterior femoral cutaneous nerve: This is a sensory nerve supplying the posterior thigh, not extending below the knee. Pain, burning, numbness, or paresthesia will be limited to the posterior thigh region when this nerve is compressed.
Inferior gluteal nerve: This nerve is predominantly a motor nerve for the gluteus maximus so weakness or atrophy of the gluteus maximus is more common than sensory sensations. It is possible that some weakness in resisted hip extension will be evident compared to the unaffected side.
Pudendal nerve: This is a mixed motor and sensory nerve so its compression produces neurological-type pain sensations felt in the perineal region, anus or genitalia as these are all areas supplied by the pudendal nerve. It also supplies muscles of the pelvic floor, so there may also be reports of bowel, bladder, or sexual dysfunction associated with the pelvic floor muscle dysfunction.
In addition to piriformis tightness from overuse or mechanical stress, some cases are caused by other factors. Other causes include blunt trauma to the area that can cause hematomas or myositis ossificans (calcification within the muscle). The hematoma or calcified tissue then presses on the affected nerve. Sacroiliac joint dysfunction can also be associated with the condition as it may cause tightness or trigger points in the piriformis due to biomechanical overload.
Vascular compression in this region may also play a part in nerve symptoms. There are arterial structures running immediately adjacent to the nerves and pressure on those can compromise blood flow to the nerves. Neural ischemia (lack of blood flow to the nerves) results and is a known cause of neurological symptoms such as pain, burning, or paresthesia sensations.
It is clear that piriformis syndrome is much more involved than simple compression on the sciatic nerve in one location. One of the key factors that makes this condition so controversial in the rehabilitation literature is that there is no gold standard for identifying it. There are some key indicators presented in this article that can be found in the client history and initial physical examination. In a future installment we’ll look at some more effective strategies for assessing and treating piriformis syndrome.
- Jankovic D, Peng P, van Zundert A. Brief review: piriformis syndrome: etiology, diagnosis, and management. Can J Anaesth = J Can d’anesthésie. 2013;60(10):1003-1012. doi:10.1007/s12630-013-0009-5.
- Hopayian K, Song F, Riera R, Sambandan S. The clinical features of the piriformis syndrome: a systematic review. Eur Spine J. 2010;19(12):2095-2109. doi:10.1007/s00586-010-1504-9.
- Michel F, Decavel P, Toussirot E, et al. The piriformis muscle syndrome: an exploration of anatomical context, pathophysiological hypotheses and diagnostic criteria. Ann Phys Rehabil Med. 2013;56(4):300-311. doi:10.1016/j.rehab.2013.03.006.